
Slower ALS progression evident with lower NfL levels: NurOwn trial
New analysis follows FDA seeing NfL drop as likely to predict benefit
Written by |

NurOwn, an experimental treatment, significantly lowered neurofilament light chain (NfL) levels in the spinal fluid, a marker of nerve damage, and this seems to predict slower disease progression in amyotrophic lateral sclerosis (ALS) patients.
That’s according to a new analysis of Phase 3 clinical trial (NCT03280056) data that examined changes in multiple biomarkers over about seven months of NurOwn’s use with in people with fast-progressing ALS.
The analysis was “motivated” by the recent U.S. Food and Drug Administration (FDA) decision to conditionally approve Qalsody (tofersen) for ALS after deeming blood NfL reductions reasonably likely to predict clinical benefit, BrainStorm Cell Therapeutics, NurOwn’s developer, stated in a company press release.
FDA allowance of likely patient benefit with lower NfL levels could impact the agency’s stance in its ongoing review of NurOwn for possible approval. Analysis findings also further support the use of NfL as a biomarker of clinical benefit in ALS, researchers noted.
FDA due to decide on NurOwn in treating ALS in early December
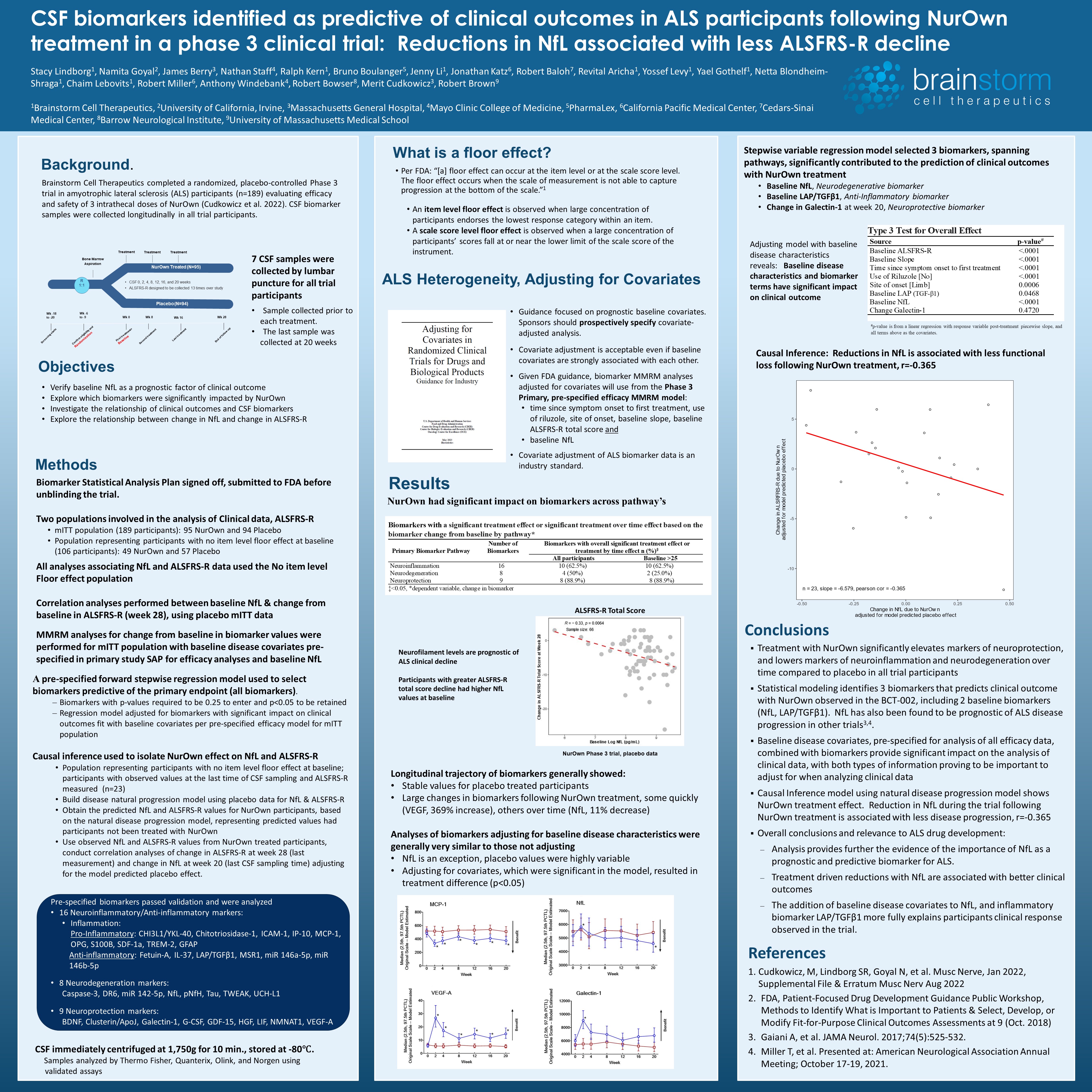
Stacy Lindborg, PhD, co-CEO at BrainStorm, presented the new findings in the poster “CSF biomarkers identified as predictive of clinical outcomes in ALS participants following NurOwn treatment in a phase 3 clinical trial: Reductions in NfL associated with less ALSFRS-R decline” at the Gordon Research Conference, held July 2-7 in Switzerland.
“The data we presented … show that it is equally important to examine biomarker data, particularly [NfL], which is a predictor of disease progression. Treatment-driven reductions in NfL are associated with better clinical outcomes in ALS,” Lindborg said.
The FDA declined to consider NurOwn’s approval request late last year, citing not enough evidence supporting its clinical benefit. After meeting with the agency, BrainStorm decided to proceed with the application filing, ensuring that an FDA advisory committee and experts will discuss the treatment’s potential.
That meeting is scheduled for Sept. 27, and a final FDA decision is expected by Dec. 8.
NurOwn is a cell-based treatment that involves taking mesenchymal stem cells from a patient’s bone marrow. These stem cells, which can give rise to a variety of cell types, are then grown in the lab to produce large amounts of molecules that help nerve cells thrive.
After being matured and expanded in the lab, the stem cells are returned to the patient via a spinal canal injection. There, they are expected to help prevent nerve cell death, slowing disease progression.
The completed Phase 3 trial included 189 patients rapidly progressing ALS, ages 18 to 60, who received three injections of either NurOwn or a placebo given two months apart.
The study’s main goal was to determine the effect of treatment on disease progression, as measured by the proportion of patients showing at least a 1.25-point slower monthly decline in ALS Functional Rating Scale-Revised (ALSFRS-R) scores over 28 weeks (about seven months).
That goal and secondary goals of mean change in ALSFRS-R scores, lung function decline, and a combined assessment of function and survival were not met.
‘Floor effect’ seen as undermining key goals of NurOwn Phase 3 trial
According to BrainStorm, these failures likely were due to a large proportion of trial participants having advanced ALS — meaning some patients at trial enrollment already would have the lowest scores on some ALSFRS-R subscales. This creates a “floor effect” that prevents changes in disease progression from being properly detected.
In line with that hypothesis, further analysis excluding patients with the lowest scores or including only those with less advanced disease showed evidence that NurOwn may slow disease progression.
The recent presentation focused on a prespecified analysis of 33 biomarkers measured in the cerebrospinal fluid (CSF), the liquid that surrounds the brain and spinal cord. Among these biomarkers, 16 were related to neuronal inflammation, eight to neurodegeneration, and nine to neuroprotection.
In general, levels of these biomarkers remained stable over time in the placebo group, but about 22 of them changed with NurOwn use.
“Treatment with NurOwn significantly elevates markers of neuroprotection, and lowers markers of neuroinflammation and neurodegeneration over time compared to placebo,” the researchers wrote.
Neurofilaments are proteins that provide structural support to nerve cells and are released to the CSF and blood when nerve cells become damaged. NfL, in particular, is commonly seem as a marker of nerve cell damage and disease progression in people with neurodegenerative conditions.
Slower ALS progression for treated patients with larger drops in NfL levels
Results showed that initial (baseline) levels of NfL in patients given a placebo significantly predicted disease progression, with higher levels being significantly associated with greater declines in ALSFRS-R scores after 28 weeks.
However, NfL levels were significantly reduced in NurOwn-treated patients after 20 weeks — the last measurement of CSF biomarkers.
A statistical model found three biomarkers that could be used to predict clinical outcomes in people receiving NurOwn, including baseline levels of NfL and the anti-inflammatory biomarker LAP/TGF beta-1, and changes in the neuroprotective biomarker Galenctin-1.
The team then showed that, after adjusting for the predicted changes due to natural disease progression, greater NfL reductions after treatment with NurOwn significantly associated with slower disease progression over the 28 weeks.
This analysis was done in the subset of patients who did not contribute to the floor effect, meaning those with scores of 1 or higher in all ALSFRS-R subscales. It “provides further … evidence of the importance of NfL as a prognostic and predictive biomarker for ALS,” the researchers concluded.

{kind=link}
Leave a comment
Fill in the required fields to post. Your email address will not be published.